
The Norwood-Hamilton Scale is the most widely used classification system for male pattern baldness (androgenetic alopecia).
Norwood Stage 3 is the first stage considered clinically significant hair loss. At this level, recession becomes clearly visible and often begins affecting confidence.
If you are Norwood 3, early action is critical — because this is the stage where strategic treatment can dramatically change long-term outcomes.
What Is Norwood 3 Hair Loss?
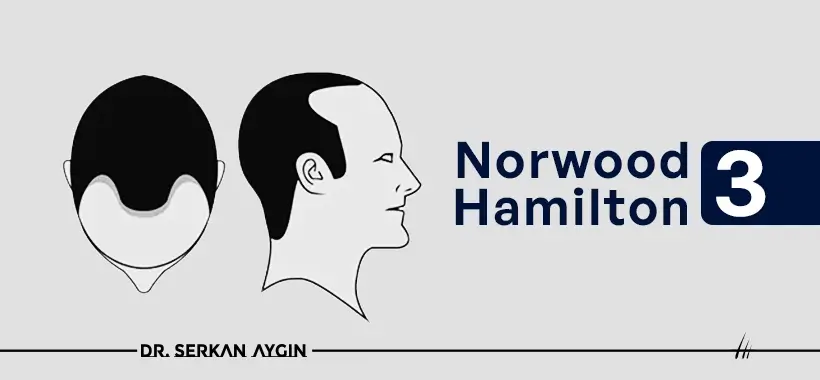
Norwood 3 is defined by:
- Deep temple recession
- Clear M-shaped, U-shaped, or V-shaped hairline
- Visible structural shift in the frontal area
- Possible early crown thinning (Norwood 3 Vertex variant)
Unlike Norwood 2 (mild recession), Norwood 3 shows pronounced hairline movement and is often the point where men actively seek solutions.
Norwood Hamilton Scale Overview

The Norwood Scale progresses as follows:
- Norwood 1: No recession
- Norwood 2: Mild temple recession
- Norwood 3: Deep frontal recession (first significant stage)
- Norwood 4–7: Progressive crown and frontal balding
Norwood 3 marks the transition from early-stage to established hair loss.
How to Recognize Norwood 3
Key Visual Indicators
- Pronounced triangular temple recession
- Strong M-shaped hairline
- Noticeable thinning when viewed from above
- Widened forehead appearance
- Possible mild crown thinning
At this stage, recession is no longer subtle — it is structurally defined.
What Causes Norwood 3?
Genetics
Androgenetic alopecia is inherited.
If male relatives experienced hair loss, your risk increases significantly.
DHT (Dihydrotestosterone)
DHT binds to androgen receptors in genetically sensitive follicles.
Over time this causes:
- Follicle miniaturization
- Thinner hair shafts
- Shorter growth cycles
- Permanent follicle dormancy
Norwood 3 reflects advanced DHT-driven miniaturization in the frontal-temporal region.
Treatment Options for Norwood 3
At this stage, treatment goals shift from pure prevention to:
- Stabilization
- Restoration
- Long-term planning
Non-Surgical Treatments
Finasteride (1 mg daily)
- Reduces DHT levels
- Slows progression
- Most effective for preserving native hair
Highly recommended to protect remaining follicles.
Minoxidil (Topical)
- Increases blood flow
- Supports follicle vitality
- Improves density
Often combined with finasteride for stronger stabilization.
PRP Therapy
- Uses growth factors from your own blood
- Stimulates weakened follicles
- Improves density
Best used as supportive therapy.
Low-Level Laser Therapy (LLLT)
- Stimulates cellular activity
- Enhances scalp circulation
- Reduces shedding
Treatment Comparison Table
Treatment | Main Action | Best For | Prescription Required |
Finasteride | Blocks DHT | Slowing progression | Yes |
Minoxidil | Improves blood flow | Thickening hair | No |
PRP | Growth factor stimulation | Density support | No |
LLLT | Follicle stimulation | Maintenance | No |
Hair Transplant for Norwood 3
For many men, Norwood 3 is the ideal stage for hairline restoration.
Why?
- Recession is clearly defined
- Donor area is typically strong
- Graft numbers are manageable
- Natural-looking results are highly achievable
Advanced Hair Transplant Techniques
FUE (Follicular Unit Extraction)
- Individual graft extraction
- No linear scar
- Minimal downtime
DHI (Direct Hair Implantation)
- Choi Implanter Pen technique
- Greater angle control
- Dense frontal packing possible
At Norwood 3, precise hairline design is critical.
Artistic planning determines natural appearance.
How Many Grafts Are Needed for Norwood 3?
Typically:
- 1,500–2,500 grafts for frontal restoration
- More if crown thinning is involved
The exact number depends on:
- Donor density
- Desired density
- Hair caliber
- Scalp elasticity
Realistic Expectations
Medical Treatment
- Slows progression
- Preserves native hair
- Requires long-term consistency
Hair Transplant
- Permanent in transplanted zones
- Results visible at 8–12 months
- New growth begins around 3–4 months
- Does not stop future native hair loss
Combining surgery with medical therapy is often optimal.
Is Norwood 3 Reversible?
- Miniaturized follicles may partially recover with medication.
- Completely bald areas require transplantation.
- Early intervention produces better cosmetic outcomes.
Long-Term Maintenance After Treatment
- Continue finasteride to protect native hair
- Consider minoxidil for density support
- Follow post-op instructions strictly
- Maintain healthy diet and low stress
- Schedule periodic evaluations
- Hair loss is progressive — planning must be long-term.
When Should You Consider a Hair Transplant at Norwood 3?
You may be a good candidate if:
- Recession is stable
- Donor area is dense
- You desire permanent hairline restoration
- You understand long-term planning
Norwood 3 is often considered the optimal stage for surgical intervention because:
- Hair loss is visible
- Donor supply remains strong
- Restoration requires fewer grafts than later stages




